The Ponseti Method is the global gold standard for treating clubfoot, offering a 95% success rate when protocols are followed precisely. Developed by Dr. Ignacio Ponseti in the 1940s, this non-surgical approach combines gentle casting, a minor tendon procedure, and bracing to achieve functional, pain-free feet. Endorsed by the Kenya Society of Orthopaedic Trauma Technologists (KESOTT), this method prioritizes mobility preservation and cost-effectiveness. Below, we break down each phase, supported by clinical evidence and insights from orthopaedic experts.
What Is Clubfoot?
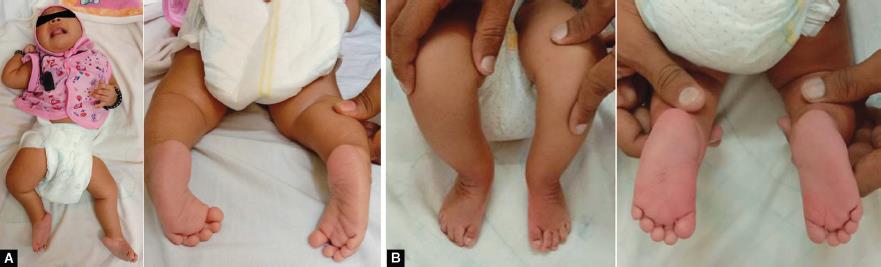
Clubfoot (congenital talipes equinovarus) is a birth defect where a baby’s foot is twisted inward and downward. Left untreated, it leads to lifelong disability. The Ponseti Method corrects this deformity without invasive surgery, making it ideal for infants and older children alike.
Why Choose the Ponseti Method Over Surgery?
1. Preserved Mobility Surgically treated feet often become stiff and painful in adulthood. The non-surgical approach retains natural joint function, enabling activities like running and dancing.
2. Cost-Effectiveness At 70% cheaper than surgical interventions, the Ponseti Method is vital in resource-limited settings.
3. Global Endorsement Recommended by the WHO, AAOS, and 35+ orthopedic societies, including KESOTT.
Phase 1: Casting – Correcting the Deformity
Timeline: 5–8 Weeks (Weekly Cast Changes) Gentle Manipulation Techniques The foot is manually repositioned to align the talus (ankle bone) as the fulcrum. Key maneuvers include:
Supinating the forefoot to correct high arches.
Abducting the midfoot outward while maintaining a downward tilt.
Note: The heel self-corrects as the midfoot adjusts—no direct manipulation is needed.
Final Cast: Addresses residual ankle equinus (tight Achilles tendon).
Achilles Tenotomy: A Minor but Critical Procedure Required in 90% of cases, this 5-minute outpatient procedure releases tendon tightness under local anesthesia. Studies show it restores ankle dorsiflexion in 98% of patients when paired with casting.
Phase 2: Bracing – Preventing Relapse
Timeline: 3–5 Years Brace Design Shoes attached to a bar, rotated outward at 60–70°.
47% experience relapse, typically due to poor bracing compliance.
Re-treatment with casting resolves 80% of recurrences.
Parent FAQs: Addressing Top Concerns Q: “What if we miss a casting session?” Delays prolong treatment. Reschedule within 48 hours to avoid setbacks.
Q: “Can older children benefit?” Yes! Success reported in patients up to age 16, per KESOTT clinical guidelines.
Q: “How to manage skin irritation under casts?” Use hypoallergenic padding and monitor for redness/swelling.
The Role of Orthopaedic Trauma Technologists
KESOTT-trained professionals are experts in:
Applying and adjusting casts with millimeter precision.
Educating families on bracing protocols.
Monitoring long-term outcomes to prevent relapse.
Global Impact of the Ponseti Method Case Study: Kenya’s Success Through partnerships with KESOTT, Kenya has reduced childhood clubfoot disability by 62% since 2015.
Common Myths Debunked Myth 1: “Clubfoot is caused by witchcraft.” Fact: It’s a congenital condition linked to genetic and environmental factors.
Myth 2: “Surgery is the only solution.” Fact: The Ponseti Method outperforms surgery in preserving mobility and reducing costs.
Conclusion
The Ponseti Method transforms lives by correcting clubfoot with precision and compassion. Backed by KESOTT, this protocol ensures children walk, run, and thrive without limitations. For more details, explore KESOTT’s resources or consult their network of certified specialists.